
Transmission of M. tuberculosis occurs mostly (with very few exceptions) via droplet nuclei which are inhaled by those who are exposed. For this reason, only those with pulmonary and/or laryngeal TB disease are likely to be contagious.
The probability of transmission varies with bacterial burden, cavitary or upper lung-zone disease on chest radiograph in the source case, laryngeal disease in the source case, exposure of bacilli to sun or UV light, amount and severity of cough in the source case, duration of exposure, proximity to source case, crowding and poor room ventilation, and delays in diagnosis, and/or effective treatment.
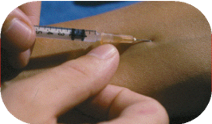 Hold skin taut. Position the bevel of the needle facing up. Insert needle intradermally at a 5-to-15-degree angle to the skin, without aspirating. The tip of the needle will be visible just below the surface of the skin. Insert the needle until the entire bevel is covered
Hold skin taut. Position the bevel of the needle facing up. Insert needle intradermally at a 5-to-15-degree angle to the skin, without aspirating. The tip of the needle will be visible just below the surface of the skin. Insert the needle until the entire bevel is covered wheal (discrete, pale elevation of the skin) should appear
wheal (discrete, pale elevation of the skin) should appear To mark the border of the induration, move the tip of a pen at a 45-degree angle laterally toward the site of the injection.
To mark the border of the induration, move the tip of a pen at a 45-degree angle laterally toward the site of the injection. Use a caliper (or flexible ruler) to measure the distance between the pen marks at the widest transverse diameter (at a right angle to the long axis of the forearm)
Use a caliper (or flexible ruler) to measure the distance between the pen marks at the widest transverse diameter (at a right angle to the long axis of the forearm)