
- Case counts (2016-2025), population estimates (2016-2023), & population projections (2024-2025): Public Health Ontario.
- Query: Case counts of reportable diseases by public health unit and year. Toronto, ON: Ontario Agency for Health Protection and Promotion; extracted on March 9, 2026.
Blastomycosis
Blastomycosis is a lung infection typically caused by a fungus that grows in moist soils, leaves, or rotting wood. It can also spread to the skin and other parts of the body.
Mushrooms, mould, and mildew are examples of fungi.
The fungus that causes blastomycosis grows as a mould in the environment, a yeast in human tissue, or as a yeast in the tissues of different mammals, such as dogs and cats.
Local Information
2025 Statistics
Incidence rate is the number of new cases of disease divided by the number of persons at risk for the disease during a particular time period.
Cases:
0*
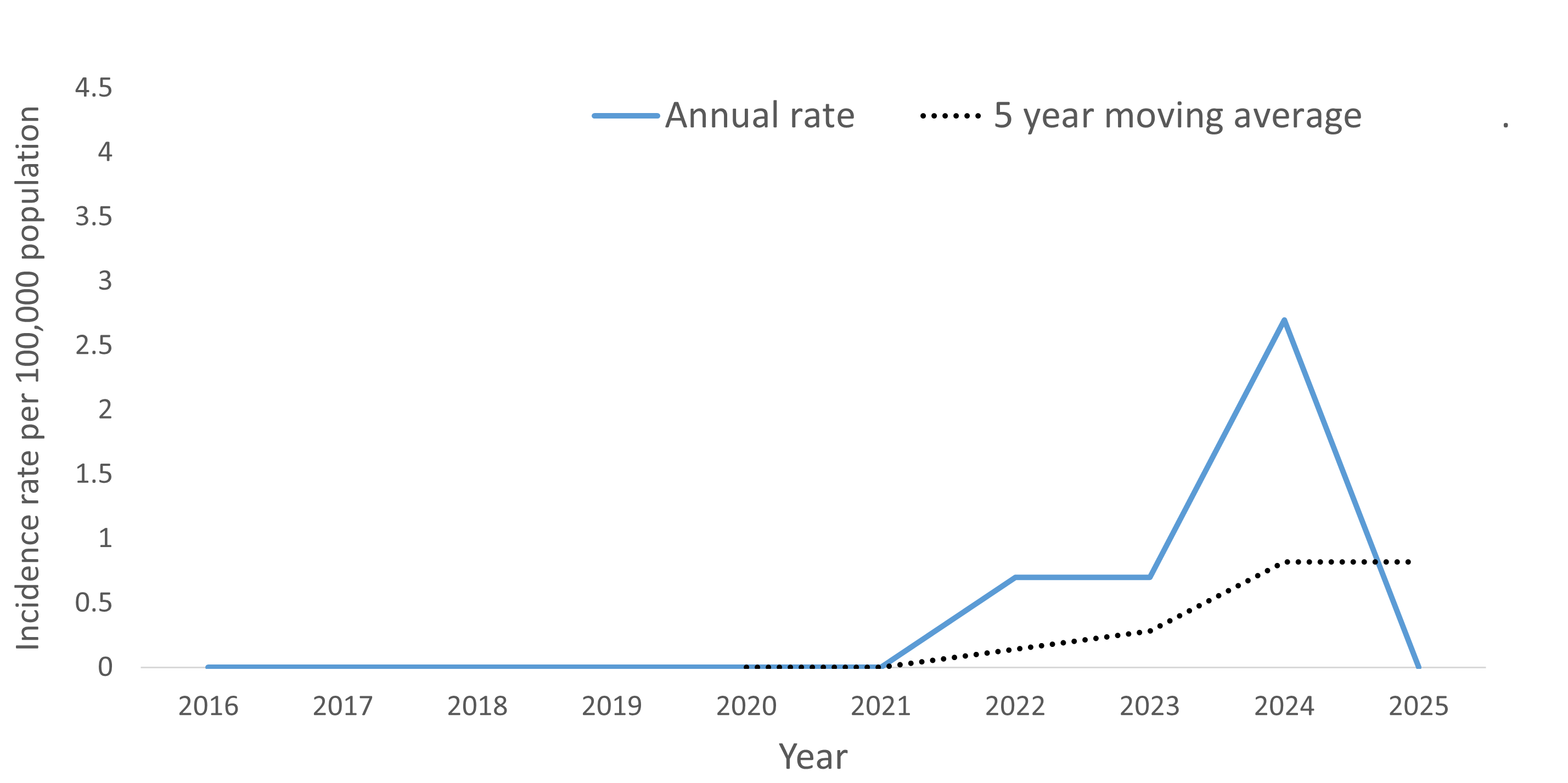
Incidence rate per 100,000 in 2025: 0
*Includes confirmed cases in 2025.
Incidence rate per 100,000 of blastomycosis by year
More information about blastomycosis
See our Blastomycosis fact sheet.
Report to the Health Unit within one business day by fax (705-482-0670) or by phone at 705-474-1400 or toll free at 1-800-563-2808, ext. 5229 if blastomycosis is suspected or confirmed as per Ontario Regulation 135/18 and amendments under the Health Protection and Promotion Act, R.S.O., c.H.7.
Should one go to childcare, school, work if they have blastomycosis?
No exclusion necessary as blastomycosis is not spread person-to-person or from animal-to-person.
Healthcare Provider Information
Blastomycosis is a fungal infection that primarily affects the lungs but can become a systemic infection with extrapulmonary manifestations. Up to 50% of pulmonary cases remain asymptomatic. Pulmonary blastomycosis may be acute or chronic.
Initial infection results from inhalation of conidia into the lungs, although primary cutaneous blastomycosis has infrequently been reported after dog bites and accidental inoculation in the laboratory or while performing an autopsy.
Acute pulmonary infection, which often goes undiagnosed, presents as an influenza-like illness with the sudden onset of fever, cough,, and a pulmonary infiltrate on chest radiographs. The acute disease often resolves spontaneously after one to three weeks. A subset of those with acute infection will go on to severe disease and acute respiratory distress syndrome (ARDS).
Chronic pulmonary infection has a slow onset where initial symptoms of cough and chest pain may be mild or absent. Clinical manifestations may include two to six months of weight loss, fever, night sweats, cough with sputum and chest pain, and may be similar to tuberculosis, other fungal infections and cancer. There is a very high mortality rate for patients who develop ARDS with chronic pulmonary infection.
Extrapulmonary disease can occur in patients with blastomycosis but is more common in patients with chronic pulmonary infection. The most common extrapulmonary site for infection is the skin (cutaneous lesions are often located on the face and distal extremities). Other common sites include bone, the genitourinary system, and the central nervous system, but any system can be affected.
It is endemic in parts of Canada, including Ontario, Manitoba and Quebec as well as several north-eastern U.S. states.
Early diagnosis and appropriate antifungal therapy are key factors in preventing morbidity and mortality related to blastomycosis. Most patients will require treatment. Treatment is indicated for all patients with progressive pulmonary or extrapulmonary diseases as well as those patients who are immunocompromised. Itraconazole is commonly used for less severe infections. Amphotericin B or amphotericin B deoxycholate are used for more severe infections, sometimes with the addition of itraconazole.
Therapeutic options for blastomycosis have been described in a guideline by the Infectious Disease Society of America. Information can also be located in the PHAC Canada Communicable Disease Report (CCDR): Perspectives on blastomycosis in Canada in the face of climate change.
Infection prevention and control
Routine practices are recommended for hospitalized cases.
If symptoms and patient activity history suggests possible blastomycosis infection, recommended tests for diagnosis include:
- Direct microscopic visualization and culture of the organism. Thick-walled, figure-eight shaped, broad-based single-budding yeast cells can be seen in sputum, tracheal aspirates, bronchoalveolar lavage fluid, cerebrospinal fluid, urine or lesional material. The gold standard for the diagnosis of blastomycosis is by culture but results can take up to four weeks. Direct microscopy can offer a more rapid diagnosis, but this method is less sensitive than culture, so a negative result does not exclude a diagnosis of blastomycosis. Where possible, submit multiple specimens for microscopy/culture over time to increase sensitivity. A poor "sputum" specimen which is mainly saliva is not an adequate specimen for diagnosis and may lead to false negative results and delayed diagnosis.
Other testing:
- Serology testing is available; however, its sensitivity is low and it is generally not recommended for diagnosing blastomycosis. Because antibodies may take several weeks to develop after exposure or infection, serology is not appropriate for acute diagnosis or for use in immunocompromised patients. While the presence of antibodies is presumptive evidence that the patient was, or is, currently infected with, or was exposed to blastomyces, serology should not be used alone for clinical diagnosis or patient management. Public Health Ontario (PHO) employs immunodiffusion (ID) as the specific assay to detect antibodies in patient serum.
- Antigen testing is not available in Canada and requires specimens to be sent to the USA for processing. It has good sensitivity, particularly in severe or disseminated disease; however, there is considerable cross-reactivity with other fungi, particularly Histoplasma, which can cause false positives. It may be suitable when collection of respiratory specimens is challenging.
Given the imperfect sensitivity and specificity of available tests, combined diagnostic approaches (including non-microbiology-based investigations) may be necessary for diagnosis.
All patients with suspected blastomycosis infection, either pulmonary or extra-pulmonary, should have a chest x-ray done to assess for lung involvement.
Refer to the following resources for additional testing information:
- PHO: Mycology - Fungal Culture - Systemic
- PHO: Fungal - Serology
- PHO's Blastomycosis in Ontario presentation
- PHAC Canada Communicable Disease Report (CCDR): Perspectives on blastomycosis in Canada in the face of climate change
Public Health Ontario:
Public Health Agency of Canada:
- For Health Professionals: Blastomycosis
- Pathogen Safety Data Sheets: Infectious Substances - Blastomyces dermatitidis
National Collaborating Centre for Infectious Diseases:
Ministry of Health: Ontario Public Health Standards:
Contact our Communicable Disease Control (CDC) program at 705-474-1400 or toll free at 1-800-563-2808, ext. 5229, or by email to cdc@healthunit.ca for more information.
Last updated: Apr 2026, by CDC